Watching a woman bleed from stab wounds until she eventually succumbed because an ambulance could not be found in time has remained etched in Judith Oketch’s mind.
The injuries were severe, and those around the scene struggled desperately to secure help. An ambulance was called, but none arrived in time. By the time assistance was finally arranged, it was already too late.
That moment changed everything for her. It was not just another emergency. It was a stark reminder that in Kenya’s fragmented emergency care system, survival can depend less on medicine and more on access, location, and speed.
She had seen a woman die because emergency help could not be accessed quickly enough. From that moment, a persistent question followed her: why is emergency response still so disjointed in a country where mobile phones and digital systems are transforming almost every other sector?
That painful experience would later shape her path and inspire the creation of an emergency response system designed to reduce delays in ambulance access through technology and an insurance-based model that connects patients to care faster, regardless of location or income.
Kenya’s emergency response system remains widely described as fragmented, shaped by decentralisation, uneven infrastructure, and inconsistent coordination across counties.
While emergency numbers exist, response times vary significantly depending on geography, traffic conditions, and availability of ambulances. In urban areas, congestion can delay response even when ambulances are available. In rural and peri-urban settings, distance and limited resources often become the biggest barriers.
For many households, particularly in low-income communities, an emergency is not only a medical crisis but also a financial shock unfolding in real time. The question of how to pay for transport often arises at the worst possible moment.
Access to an ambulance is often uncertain. In some cases, it is unaffordable. In others, it is simply unavailable.
This gap between need and access is what emerging private-sector innovations are attempting to address.
Through a partnership model involving county governments and private sector providers, Ambulex Solutions has introduced a subscription-based ambulance service designed to improve emergency response access.
Under the system, households pay as little as Sh200 per year to access emergency ambulance care. Once registered, users can request an ambulance through a mobile application or USSD code, which connects them to a digital dispatch platform that identifies and assigns the nearest available unit.
 Judith Oketch explaining how the model works. (Photo: Handout)
Judith Oketch explaining how the model works. (Photo: Handout)
The system is designed to function much like a ride-hailing platform. Instead of passengers and drivers, it matches patients with ambulances based on proximity, availability, and urgency.
“The system identifies the nearest ambulance and dispatches it immediately,” says Judith Oketch, who leads the organisation. “In emergencies, time is the difference between life and death.”
For non-subscribers, services are charged at market rates, which can range from a few thousand shillings to over Sh100,000 depending on distance, urgency, and complexity of care required during transport.
The model is built on risk pooling, where many households contribute small amounts to ensure that emergency services are accessible when needed.
The organisation now operates a network of more than 270 ambulances across Kenya, with Nairobi accounting for about 100 units. It estimates it has responded to more than 10,000 emergency cases and serves hundreds of thousands of subscribers.
Behind the system is a coordinated network of dispatch teams, paramedics, drivers, and partner ambulance providers working around the clock. The system relies heavily on digital coordination, GPS tracking, and real-time communication between responders and dispatch centres.
However, even with this infrastructure, ambulances alone cannot always reach patients in time, especially in informal settlements or hard-to-reach areas.
In densely populated informal settlements and rural areas with narrow roads, congestion and poor infrastructure often delay emergency vehicles.
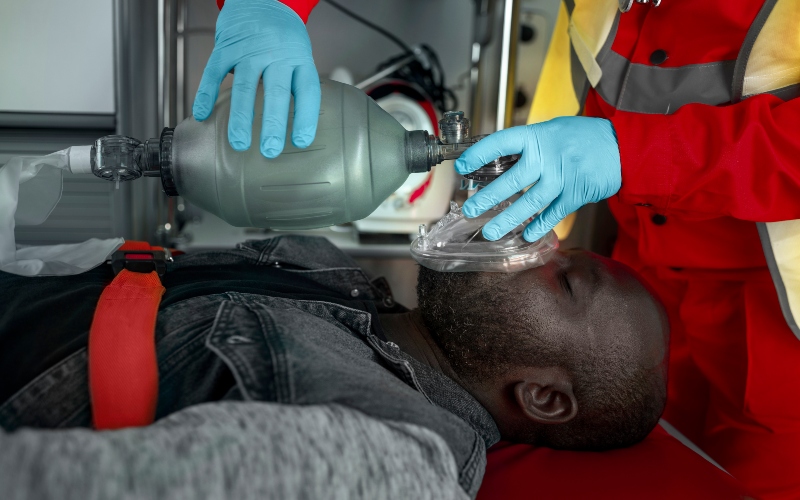
To bridge this gap, motorbike-based emergency medical technicians (EMTs) equipped with trauma kits are deployed to reach patients first.
These first responders are trained to provide immediate stabilisation before evacuation.
“In areas where ambulances cannot enter, EMTs go in first to stabilise the patient,” Oketch explains. “Once the patient is stabilised, an ambulance is dispatched if needed.”
This creates a two-layer emergency response system: rapid first contact at the community level, followed by ambulance evacuation when necessary.
It is a model designed to address one of the biggest weaknesses in urban and rural emergency care, delayed access in high-density areas.
In emergency medicine, time is not just important; it is decisive. Survival rates for trauma, stroke, cardiac arrest, and obstetric emergencies often depend on how quickly care begins.
The system is therefore designed around speed and proximity.
 An ambulance. (Photo: Freepik)
An ambulance. (Photo: Freepik)
“The most important moment is reaching the patient,” Oketch says. “Once they are stabilised, transport becomes safer and more controlled.”
The approach shifts emphasis from transport alone to early intervention, ensuring that care begins before the patient reaches a hospital.
While much attention is given to equipment, vehicles, and response times, emergency care is also emotionally demanding for frontline workers.
Responders regularly encounter traumatic scenes of road accidents, violent injuries, maternal emergencies, and sudden deaths.
Oketch says supporting the mental health of responders is essential to sustaining the system.
“You cannot run emergency services without caring for the people who respond,” she says. “If they are burned out, everything breaks.”
To address this, the organisation incorporates debriefing sessions after critical cases, allowing teams to process experiences and reflect on outcomes. There are also ongoing efforts to strengthen structured psychological support for staff exposed to repeated trauma.
Not every emergency ends in survival. Even with rapid response, some patients arrive too late or in conditions beyond medical intervention.
Oketch acknowledges this reality with clarity.
“Yes, we have lost patients en route,” she says. “It is painful, but we always go back to ask whether protocols were followed, whether it was a system failure, or whether the case was already beyond survival.”
Rather than focusing on blame, the organisation emphasises continuous learning and system improvement.
“In healthcare, mistakes happen. What matters is whether you learn from them and improve the system.”
This culture of reflection is central to emergency medicine, where decisions are made under pressure and outcomes are not always predictable.
Despite growing adoption, challenges remain in public understanding of ambulance services.
Some patients, after receiving emergency transport, refuse to pay or question charges.
“There are cases where people say, ‘Did I ask you to come?’ even after we have rescued them,” Oketch says.
Such responses reflect a broader gap in public awareness about pre-hospital emergency care and how it is funded, especially in systems where private providers play a significant role.
For many communities, ambulances are still seen as optional transport rather than critical medical services.
To improve awareness and access, the system works with county governments, community health promoters, Nyumba Kumi structures, and grassroots organisations.
Outreach efforts include door-to-door campaigns, medical camps, and community education programmes aimed at informing households about emergency response options.
 Judit Oketch, founder of Ambulex solution. (Photo: Handout)
Judit Oketch, founder of Ambulex solution. (Photo: Handout)
At the same time, EMTs stationed within communities act as local first responders, reducing response times in underserved areas and building trust through familiarity.
These local networks are particularly important in informal settlements, where trust in formal systems can be low, and response delays are historically high.
As Kenya’s urban population grows and pressure on health systems increases, this model represents a shift toward tech-enabled, community-linked emergency care where survival is not determined by income, distance, orchance butt by timely response.
It is still evolving, shaped by operational realities, partnerships, and lessons from the field. But for many households, it has already become the difference between waiting and being saved.
For Yvonne Mutiso, the system became real in a moment she never expected.
She first learned about the service at a health facility, where she registered and paid a subscription fee of Sh200, not imagining she would ever need it.
A month later, her daughter went into emergency labour in Kitengela after she began bleeding unexpectedly at home. With no immediate transport available and the situation escalating, Yvonne panicked and called the emergency number she had been given.
An ambulance arrived in about 20 minutes. The team provided immediate first aid, including vital checks and stabilisation, before transporting her to the hospital.
“I had never called an ambulance before, and I didn’t think they would come. But they did, and that made all the difference.”
At the hospital, she received further care and was later delivered safely, without complications.
For Yvonne, what had once seemed like a low-cost optional subscription became a lifeline in one of the most frightening moments of her life.













































Comments
Sign in with Google to comment, reply, and like comments.
Continue with Google